
A 750‑bed teaching hospital located in a major US city is filled beyond capacity—again. 没有住院床位. 医院被迫让病人住在走廊和手术康复区. 其急诊科(ED)已被转移, 将运送非创伤病人的紧急运输工具送到该地区的其他急诊室.
这样的场景在许多医院都很常见, 尤其是在城市地区, 病人担心他们需要的云顶集团是否能得到. 医院关心的是保持质量, 改善患者体验, 尽量减少对底线的影响.
Experts have warned that more and more hospital beds will sit empty as payers push for care to be provided in less costly settings. 但如果住院病人数量呈下降趋势, 为什么许多医院都在争先恐后地寻找额外的床位?
利用的转变
利用数据表明,很大一部分患者数量并没有下降, but shifting: observation patients are frequently held in inpatient units and cared for by unit nurses. 结果是, fewer beds are available for inpatient admissions from the ED or for those recovering from surgery.
这一趋势给医院领导带来了战略困境. 从设施和资本规划的角度来看, 床位短缺的医院必须决定是否投资新床位.
医院应该投资新床位吗?
随着医院采用新的护理模式, 可能会有更少的观察患者在医院得到照顾. 例如, telehealth gains seen during the COVID‑19 pandemic have shown that patients could be monitored in their homes with proper outpatient follow-up. 另外, visiting clinicians can provide support to patients recovering from surgery in their homes or hotel-like settings. 考虑到这些趋势, hospitals have options beyond adding inpatient capacity to address an inefficient use of unit beds—especially since demand for bed capacity continues to evolve.
医院必须打好基础.g., 护理管理结构, 技术, 以及数字能力),以便在更便宜的环境中安全地照顾病人. This is quickly becoming a financial necessity, and some would argue a moral obligation. 进一步, 替代支付结构正变得越来越普遍, 使提供商组织面临在医疗费用总额中承担更大份额的风险.
许多医院现在需要观察床位,在可预见的未来也需要. 投资一个或多个专门的观察单位可以产生积极的投资回报率. 一项研究 显示医院建立观察室可以节省1美元,平均每个病人572, representing revenue in addition to that obtained by freeing specialized-care beds for patients who need them. Additional cost efficiencies can be achieved by aligning the appropriate level of clinical staff per patient.
然而,关键是要确保这一点
设施设计足够灵活,可以根据日常、季节性、
或者紧急情况.
深入研究利用率
利用率数据进一步揭示了这个问题. Across the US, there is a decline occurring in inpatient volumes, as many have predicted. National inpatient use rates have decreased at a compound annual growth rate (CAGR) of 1.自《云顶集团40011官网》签署成为法律以来,这一比例为0%. 住院人数从2010年的每千人114人下降到2015年的104人到2019年,一直在103到105之间停滞不前.
研究还表明,24小时以上的观察时间显著增加. 在医疗保险患者中,住院人数增加了22%.1%,从2011年到2013年, a 10.5%的复合年增长率. 这一趋势至少持续到了2014年, and the trend is directionally true for patients on commercial plans too (although the growth is not as rapid), 如下所示.
当我们一起研究时,这些趋势说明了什么?
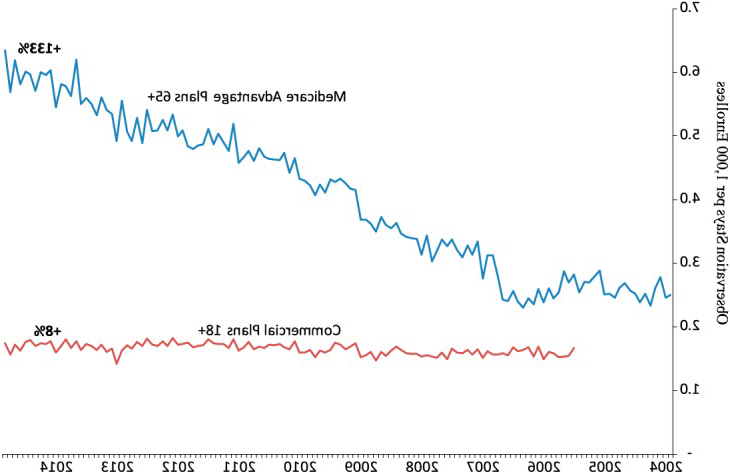
根据医疗保险支付咨询委员会 分析 40%的住院病人 下降的原因可以解释为住院患者被分类为以下 观察而非承认. 这是一个相当大的比例,这很有帮助 解释为什么许多医院在已有能力的情况下还在探索增加能力的必要性 计划裁员. 从战略角度来看,注意这一点很重要 60%的住院人数下降不能用转为观察来解释. 的 门诊治疗的趋势仍在发生,只是没有一些人那么快 统计数据显示.
观察床位与住院床位
而观察患者被所有支付方视为门诊患者, 他们经常在医院呆上一两个晚上. 但是他们需要什么样的床呢?
It’s helpful to compare the different resource and space needs for inpatient beds versus observation beds. 住院病房往往是私人的, 占地面积大(按当代标准净面积260至300多平方英尺), 而且大多数都有浴室. 观察床对空间和配置的要求不那么严格. 虽然医院领导希望给观察病人一个舒适的环境, 特别是考虑到重新关注以病人为中心的护理和满意度, the accommodations do not have to be as comprehensive—or expensive—as inpatient rooms.[1]
灵活的设施空间
A solution for addressing capacity constraints is to develop a dedicated observation unit to care for short-stay patients who do not meet the criteria for admission as an inpatient, 但在出院前需要长期护理. This option dictates resources and design that match the specific needs of these patients, 包括适当的人员配备水平, 空间配置, 功能性邻接. 与此形成鲜明对比的是, observation patients who are placed in inpatient units can end up staying in the hospital for longer than necessary, 他们的护理方案不太统一, 而且管理成本更高.
并非所有的观察患者类型都是相同的. 分类有以下几种:
- 在急诊科做出的临床决定.
- 一般医学观察.
- 术后长期恢复.
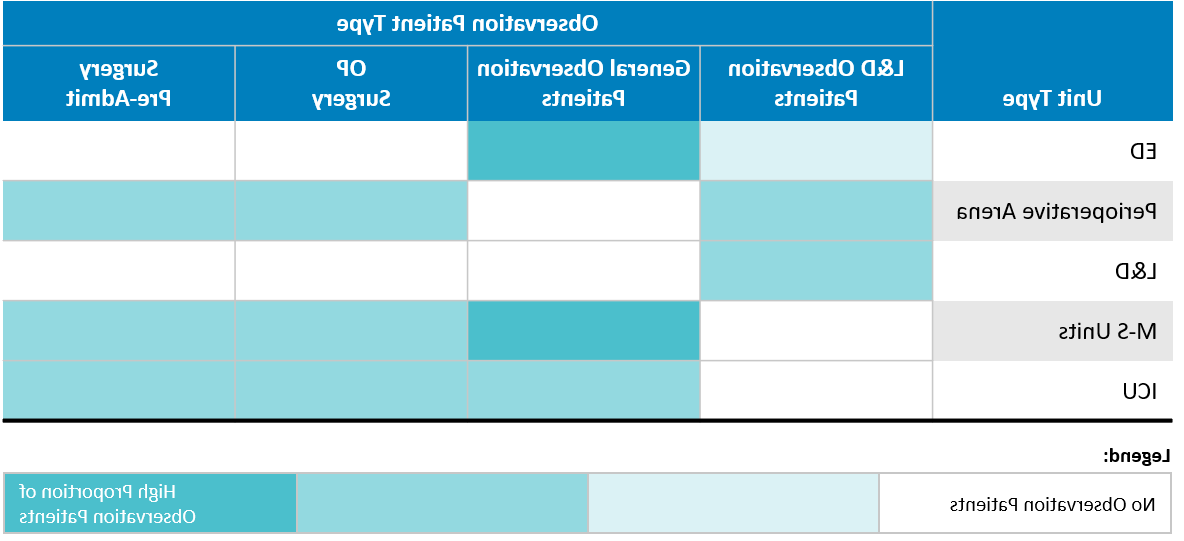
(医院云顶集团40011官网和急诊科云顶集团40011官网), 空间可用性, 以及对急诊科治疗室和住院病床的需求程度, 如下图所示.

的信息样本
学术医疗中心,在下表中,显示了他们的观察
病人在没有观察室(或多个病房)的情况下被安置
这些病人的不同需求. 心脏外科
(M-S)和重症监护病房(icu)治疗了高比例的患者
观察床外的急诊科,而分娩(L&D)患者
在专门的L&D单位.
Finding space for a new bed unit can be difficult; many hospitals in urban settings are facing capacity constraints. But additional options can surface when the smaller space requirements of an observation unit are considered. Several hospitals that were experiencing capacity constraints have been implementing observation and extended recovery beds in quantities equivalent to approximately 5% to 10% of their total inpatient bed capacity. 这个百分比取决于具体的市场动态, 住院设施的规模和云顶集团组合, 云顶集团40011官网保险, 除其他因素外. 除了, 观察床应考虑商业占用分类, 尤其是门诊手术, to further reduce the costs and space constraints typically associated with buildings that are designed for inpatient occupancy.
有一个可扩展的设施计划很重要, 特别是随着门诊治疗模式的不断扩大和变得 根深蒂固的. 为了帮助减轻财务风险,应该设计一个观察单位 灵活地适应不同类型的患者. 为 例如,在ed附近建造这些单位通常是个不错的策略. 大多数观察患者来自急诊科,可能由急诊科工作人员照顾, 并且这些单元可以很容易地转换为额外的ED治疗空间 需求出现了. 与程序相邻的观察单位也是如此 恢复门诊或门诊空间,为其提供逻辑扩展路径 这些云顶集团.
规划未来
的 recent census swings associated with the COVID‑19 pandemic have crystallized our thinking about how a medical center can best adapt to a sudden and perhaps prolonged influx of complex, highly infectious patients—how to triage and segregate patients based on their condition, 把病人放在哪里最好, 以及如何管理员工和资源. It can be challenging to balance near-term space needs with longer-term goals and projections, 观察单位, 就其本质而言, are adaptable investments for healthcare organizations to accommodate a multitude of bedded patients.
通过设计可扩展的, 为观察患者提供灵活的病房, inpatient care centers—from rural community hospitals to urban academic medical centers—can meet immediate revenue goals, 为他们的社区提供及时的护理, 为未来的需求做好准备.
脚注
- 1.
要按照2018年FGI指南,每个 病房必须有自然光,通过窗户向外照射 除其他要求外,私人病人厕所.
出版于2021年12月7日